Chest X-Ray Analysis: Effusion, Oedema, and Pneumonia
Posted on Jul 7, 2026 in Medicine
1. Pleural Effusion
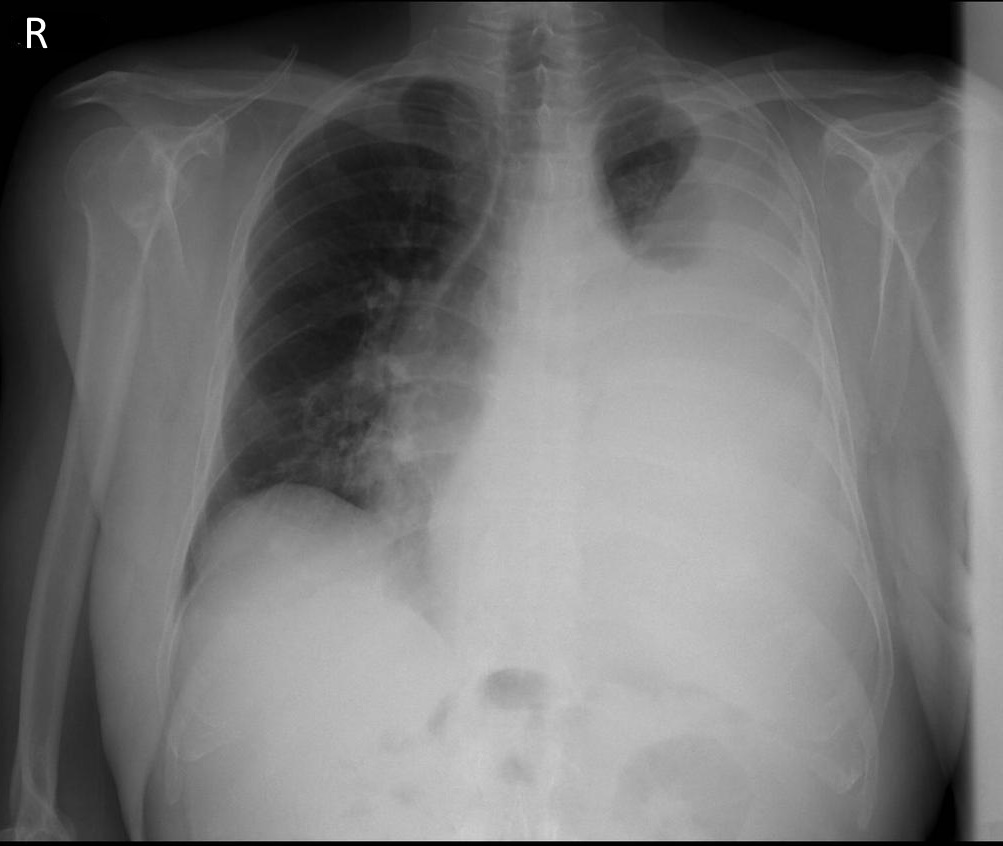
Interpretation
- Quality: RIPE – Good
- 1. Airways: Trachea deviated to the right (pushing effect because of effusion); cannot visualize the carina or bronchus.
- 2. Breathing: Effusion in the left lower and middle zones which ends in the upper zone with a meniscus sign; lung markings present throughout the right lung.
- 3. Cardiac: Cannot assess the size; difficult to visualize left heart borders.
- 4. Diaphragm: Right hemidiaphragm can be seen; left cannot be seen; blunting of the left costophrenic angle; right angle is sharp and visible.
- 5. Everything Else: No fractures; no changes in soft tissues.
Clinical Questions
- Differential Diagnosis: Unilateral pleural effusion (focusing on causes of pleural effusion).
- Investigations: 1. CT thorax; 2. Pleural aspiration to determine if it is an exudate or transudate; cytology for cancerous cells; microbiology for infection.
- Fluid Classification: How would you determine if the fluid was a transudate or an exudate? Using Light’s Criteria.
2. Pulmonary Oedema
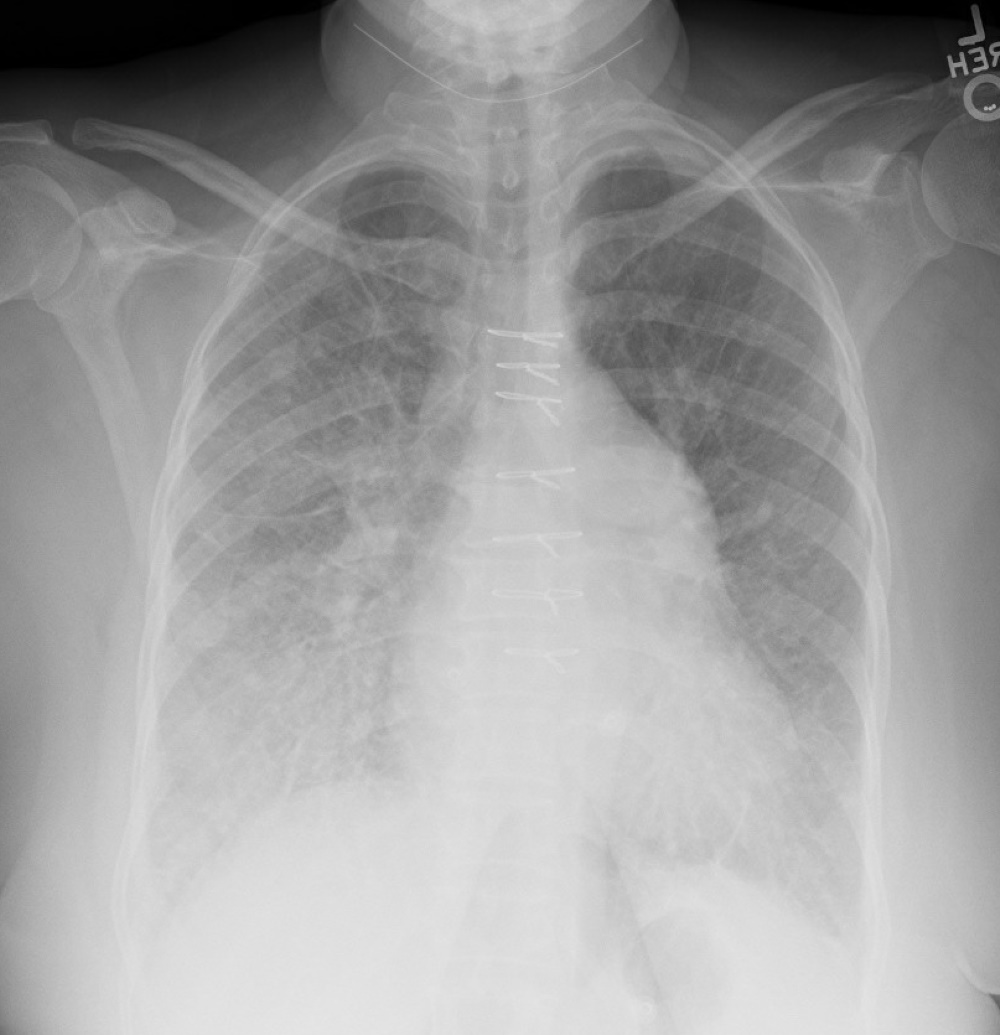
Interpretation
- Quality: RIPE – Good
- Airway: Trachea is central; carina, Right Main Bronchus (RMB), and Left Main Bronchus (LMB) are visible; right hilum present but left hilum is obscured.
- Breathing: Bilateral perihilar shadowing present; Kerley B lines visible. No pleural thickening or abnormalities found.
- Circulation: Heart borders visible; enlarged cardiac diameter (cardiomegaly).
- Diaphragm: Not flattened; gastric bubble can be seen.
- Everything Else: No fractures or soft tissue abnormalities; several midline sutures are present.
Clinical Questions
- Findings and Diagnosis: Important findings include: a. Bilateral perihilar shadowing (alveolar oedema with a bat wing appearance); b. Kerley B lines; c. Cardiomegaly (enlarged cardiac diameter). Diagnosis: Pulmonary oedema.
- Investigations:
- ABG: To look for hypoxia.
- Blood Tests: FBC, U&Es, LFTs (baseline and check for hypoalbuminaemia), Troponin (to rule out ACS), and BNP (for heart failure).
- ECG: To look for myocardial infarction or ventricular hypertrophy.
- Echocardiogram: To diagnose heart failure and assess ejection fraction (if it is a first presentation).
- Immediate Management:
- Oxygen: Maintain O2 saturations at 94-98%, or 88-92% in CO2 retainers such as those with COPD.
- Diuretics: IV furosemide; for severe cases not responding to diuretics, consider vasopressors, inotropes, or nitrates (requires specialist input).
- Positioning: Sit the patient upright.
- Fluid Balance: Maintain a fluid balance chart to ensure the correct amount of fluid is being excreted.
3. Pneumonia and LRTI
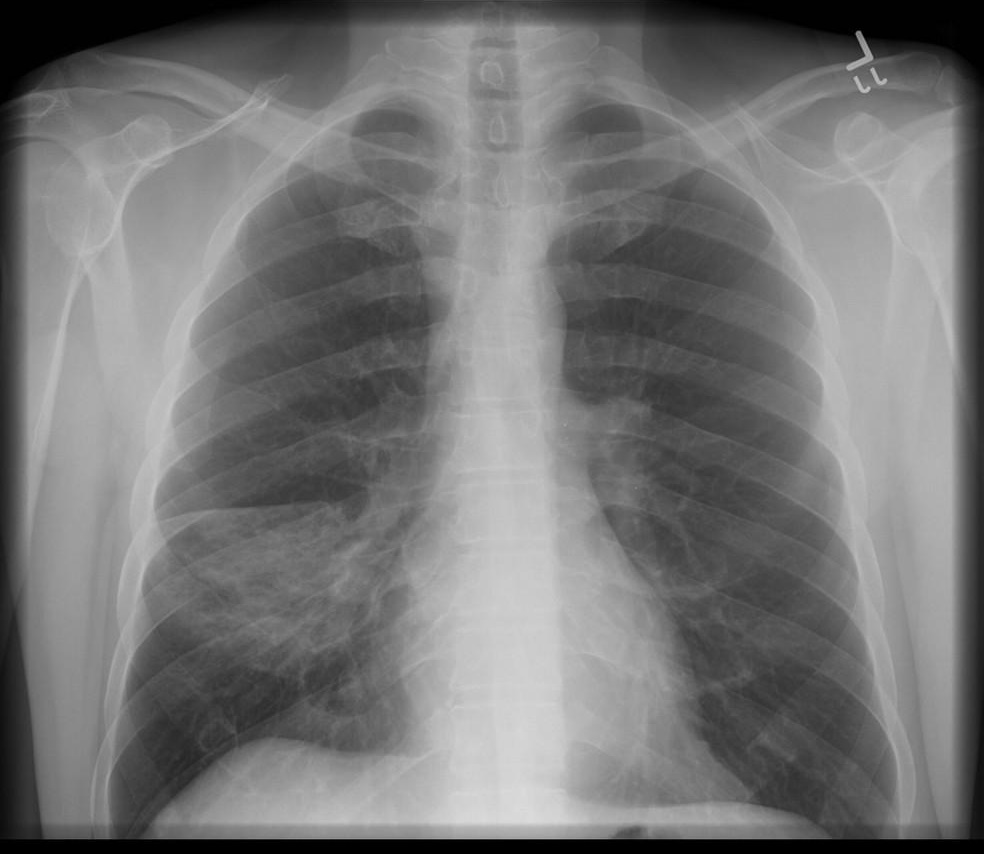
Interpretation
- Quality: RIPE – Good
- Airways: Trachea central; carina, RMB, and LMB visible; right and left hilum visible.
- Breathing: Right lower-mid zone opacification consistent with consolidation; borders of opacification are ill-defined. Left lung is normal with the presence of lung markings; pleural margins show no thickening or abnormalities.
- Cardiac: Normal heart borders; cardiothoracic ratio < 0.5.
- Diaphragm: Not flattened; right and left hemidiaphragms are visible; gastric bubble can be seen; no air under the diaphragm. Right and left costophrenic angles and cardiophrenic angles are visible.
- Everything Else: No fractures; no soft tissue abnormalities.
Clinical Questions
- Diagnosis and Differentials: Most likely: Pneumonia. Differentials: Lung cancer, Pulmonary Embolism (PE), Pulmonary oedema, or Aspiration.
- Investigations:
- Bedside: Full set of vital signs, ECG, and urine dipstick.
- Bloods: FBC, CRP/ESR, baseline U&Es, LFTs, blood cultures, and sputum samples.
- Other Tests: HIV testing, TB screening, or screening for other respiratory viruses based on history and clinical presentation.
- Management:
- Calculate the CURB-65 score to guide management.
- Antibiotics: Empirical antibiotics based on the likely organism and allergy status.
- Oxygen: Administer if needed.
- IV Fluids: If there is evidence of dehydration or shock; balance carefully to avoid fluid overload.
- Supportive Care: Analgesics and antipyretics.
- Admission: Consider hospital admission for patients with severe pneumonia, those requiring IV antibiotics/fluids or oxygen therapy, patients with underlying health conditions, or those who cannot be managed via outpatient treatment.